


Health sector demonstrates the incredible power of the "system"
Abook published a decade ago by the United Nations (2005) titled “Public Enterprises: Unresolved challenges and new opportunities” stated that the performance of public enterprises is determined 80 percent by the system, 16 percent by the leadership and only four percent by rest of the staff. Before 2008, the eHealth and the health information infrastructure of Bangladesh's government healthcare network did not pay much attention to building a good system as well as providing appropriate leadership. Since mid 2008, the approach and design of the country's health information system (HIS) has been redefined, boosted by the extensive political support of Digital Bangladesh Vision 2021. The progress of eHealth and the electronic health information system of Bangladesh has drawn significant global attention; they are being recognised as models to follow in other countries.
The most recent recognition came from the German government through the formal launching of a book titled “A quiet revolution: Strengthening the routine health information system in Bangladesh” by its Federal Ministry of Economic Cooperation and Development in Berlin (November 26, 2014). The book summarises the results of HIS strengthening in Bangladesh into five broad categories, viz., i) dramatically reduced administrative burdens - and more time for patients - through digitisation of routine reporting; ii) use of individual health records improves patient care; iii) a national electronic repository signals the end of information silos; iv) better quality and more comprehensive routine information now available from the public sector; and v) improved capacity at Bangladesh's Ministry of Health and Family Welfare and growing international contributions in eHealth. In 2011, the Honorable Prime Minister Sheikh Hasina received the United Nations South-South Award for Digital Health. The Management Information System (MIS) of the Directorate General of Health Services (DGHS) under the MOHFW of Bangladesh could make this success happen in just a few years.
The background
In early 2008, the office building of the MIS department of DGHS doned a gloomy frustrating look due to poor maintenance for years at a stretch. There was no internet connectivity, not even in the head office. Work environment, in respect to light, ventilation, sitting arrangement, ICT resource, staff skill and motivation, was also very poor. Staffs were unskilled and frustrated due to the lack of career prospect. Data collection was conducted using paper forms and would take, on average, two months from the lowest level health facilities to the MIS department. Now things have changed and data flows instantaneously and electronically. There has been significant improvement in physical and ICT infrastructure, training, skill and staff motivation, monitoring, supervision, transparency and accountability, and data quality and information culture as a whole.
 For all latest news, follow The Daily Star's Google News channel.
For all latest news, follow The Daily Star's Google News channel. Motivation for change
The mandate, available strengths, weaknesses and opportunities of the MIS department were revisited in 2008. It was revealed that without the use of ICT, management and meaningful use of health data from across thousands of health facilities and organisations all over the country would not be possible. A blueprint was made for gradually building an ICT-based national HIS infrastructure and system to make the best use of health data. In 2009, the effort received enormous political support due to the government's Digital Bangladesh Vision 2021. An eHealth component was also added on top of the HIS. Today's progress is the result of the consistent effort to improve and implement the blueprint.
Full internet connectivity of health sector
The MOHFW of Bangladesh started connecting health organisations to the Internet in May 2009 and completed connectivity of the entire health sector by April 2014. The 24,000 rurally deployed frontline health workers engaged for home visits, about 13,000 community clinics, all the union health centers and all public hospitals, academic institutions and health administrative offices (all together about 1,000) now have tablet PCs, laptop computers, desktop computers or computer LANs, as appropriate. Connectivity, principally, is provided by broadband wireless modems (3G if available locally, otherwise 2G). A state-of-the-art data center in the MIS office in Dhaka and a disaster recovery system in the Khulna health office have been established. All MOHFW staffs, responsible for handling and using ICT, have been trained.
Software solution - eHealth enterprise architecture - citizens' lifetime electronic health records
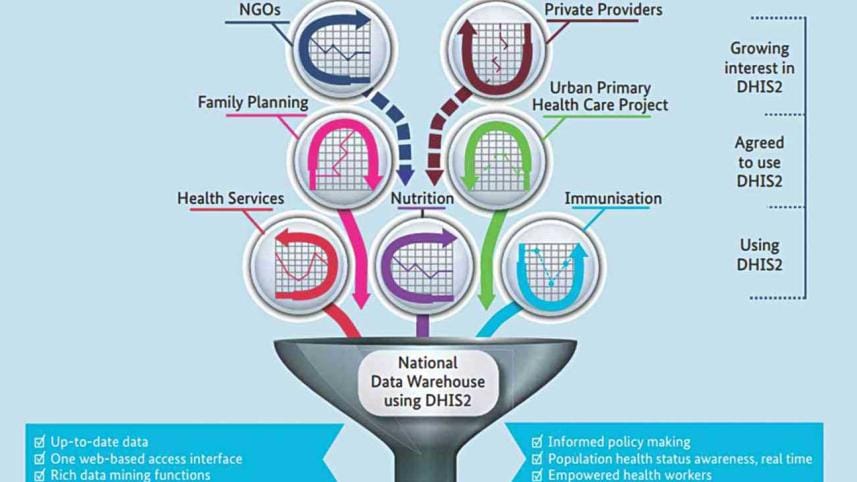
To enable health staffs with sufficient ICT skills to perform eHealth-related work better, use of too many softwares was discouraged. Only three web-based open source softwares, viz., DHIS2, OpenMRS and HRM, have been chosen for all kind of situations. The DHIS2 (District Health Information System, version 2), developed in the University of Oslo, Norway, is used for gathering data on preventive and public health services from all over the country and is being applied by both state and non-state healthcare providers OpenMRS (Open Medical Record System), a globally acclaimed software, has been chosen for hospital automation. The HRM (Human Resource Management) System has been developed in-house and is used for processing human resource information. Multimedia projectors have been provided to each upazila, district and divisional health manager's office to enable them hold monthly review meetings with the help of software-generated automated reports. Another breakthrough that will be introduced by the end of 2015 is the electronic shared health records (SHR) system. The SHR will be portable between healthcare providers and hospitals for real-time reference and updating. To take this implementation forward, the MIS has already collected electronic records of 98 million citizens. The SHR will integrate the DHIS2, OpenMRS and HRM in an eHealth enterprise architecture (eHEA), to exchange data through an electronic health information exchange (eHIE). MIS is also working with a multi-ministerial initiative led by the Cabinet Secretary to develop an electronic universal civil registration and vital statistics (CRVS) system to lead to an electronic national population register (NPR) with a view of making a national citizen registry with a core basic data set to authenticate each individual with unique identification and biometric data. The MIS has already made a rich data source for geo-locations, health organisations and health workforce in the form of electronic registries.
Citizens' grievance management system: complaint-suggestion box
In 800 public hospitals and organisations, there are display boards mounted on walls, which describe how to send complaints about the quality of services or suggestions for service improvement. Clients of the hospitals or health organisations text complaints or suggestions to a particular mobile number shown in the display board. According to the DGHS website, a web server located at MIS receives the texts and makes them available instantly for public viewing. The responsible staff members at MIS check the complaints and suggestions, talk to the SMS senders to find out more about the message, and undertake actions to solve the problem or work on the suggestion. The complaints and suggestions become publicly available in real time on the DGHS website.

Mobile phone health service
All upazila health complexes and district hospitals (a total of 482) provide medical consultation free of cost through mobile phones. Each of the hospitals has a mobile phone carried by an on-duty doctor. This phone is accessible for incoming calls round-the-clock. People living in the catchment areas call the number, if the need arises, and the doctor gives appropriate medical advice. The service has been extended to about 13,000 community clinics The mobile phone health service received the ICT4 Development Award in 2010 and special mention at the Manthan India Award in 2011.
Telemedicine
In 42 government hospitals, advanced telemedicine centers have been established. Equipped with different remote capture peripherals and dedicated bandwidth, these centers are providing referral specialist consultations to patients attending the peripheral hospitals. The community clinics in rural Bangladesh also take advantage of internet connectivity for patients who require direct medical advice from a qualified doctor working either at upazila or district hospitals. They communicate via video-conference over Skype to help link doctors and patients.

Office attendance monitoring from central point by fingerprint machines
Allegation about staff absenteeism particularly from remote health facilities is not uncommon. The MIS installed low cost fingerprint time attendance machines in all upazila and district hospitals. Staffs record their check-in and check-out times by touching the sensor of the respective machine. The office attendance data is then transferred to the central server via the Internet and becomes available for viewing from anywhere through a web portal. Daily, weekly, monthly and yearly staff attendance reports can be produced for national, subnational and local levels.
ICT and local health interventions - improving maternal and child health through COIA initiative
Under an initiative launched by the United Nations called COIA (Commission on Information and Accountability) for maternal and child health, the MIS started to electronically register and track every pregnant woman and under-five child, using 11 core indicators. All partner healthcare providers use a shared electronic online data collection form in DHIS2 for this purpose. Frontline health workers and community clinics register pregnant women and under-five children living in the respective community catchments by using this online form. A routine weekly meeting is held at the community clinic, where government, NGO health workers and members of the community clinic management committees jointly review, validate and clean collected data to measure and understand the local maternal and child health situation, make intervention plans and implement those in the next week(s), taking up shared responsibility. Automatically generated summary reports in the form of lists, tables, charts and maps from DHIS2 make the review simple and easy. Review by the higher authorities is also done and feedback is given. This routine “Monitor-Review-Act” cycle continues and thereby local communities take control of their own maternal and child health situation.
Interactive online health bulletins
An exciting work of the MIS is the introduction of an interactive web-based publication called the “local health bulletin” by each health organisation under DGHS. Local health bulletins have created an opportunity to obtain local health data on the upazila, district or hospital level; they are also helping to build local information culture. Over 500 government health organisations publish their own health bulletin using a web-based template provided by MIS. Each organisation prints hard copies of their own local health bulletin and organises a local annual publication ceremony before the national annual health MIS conference; at the national conference, local managers and allied staffs present and defend their respective local health bulletins. Such interventions help to improve the quality of data of local health bulletins and contribute to the strengthening of local information culture.
Multiple stakeholders sharing the same health data platform
The success of the MIS is owed to the creation of an environment which harbors the convergence of all vertical health programs and health stakeholders into one shared HIS resource (data center and DHIS2) for collection and use of health data. Vertical programs like community clinics, maternal and child health programs, etc., are all using the same resource. Development partners like the World Bank, GiZ, DFID, UNICEF, ICDDRB, USAID, JICA, SAVE, UNFPA, PLAN, CIDA, SIDA, BRAC, JHU, etc., are supporting and/or using the system.
The use of social media platforms
The web portal of MIS remains as a vibrant platform for health information dissemination. The website has been completely redesigned to accommodate new trends and tastes. Social media interfaces, viz. Facebook, Twitter, Google+, YouTube Channel, etc. are being successfully used to attract a wide range of audiences. Our social media platforms are attracting the largest number of audiences, about 500,000 each month.
Public-Private Partnership - mHealth for safe pregnancy and childcare
MIS is carrying out a partnership program with D.Net (supported by USAID) to provide a mHealth service called MAMA (Mobile Alliance for Maternal Action). The program uses a short telephone code (16227), which provides to pregnant and new mothers, lifesaving information and advice for newborn babies and children through SMS and IVRs. MIS is also working with WHO and Johns Hopkins University to develop and operate mCare (for pregnancy care), mTikka (for immunisation) and OpenSRP (for easy data entry by frontline workers).
Conclusion
The Bangladesh Ministry of Health and Family Welfare is enjoying the benefits of building a system rather than an ad hoc solution for health information and eHealth. The simple, low cost, yet effective solution has drawn remarkable global attention as an eHealth model. The eHealth system is generating evidence for decision-making, improving health system efficiency and quality, helping the ministry to reach the citizens with service, and bridging the urban-rural digital divide. The nationwide unified eHealth network has just started to reveal its incredible power to transform public health through mass empowerment, particularly that of grass-root actors.
..............................................................
The writer is Additional Director General and Director of Management Information System (MIS), Directorate General of Health Services (DGHS)
Comments