Human Rights analysis
Right to have proper medical care
Oli Md. Abdullah Chowdhury
The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, social and economic condition. Elites though prefer taking resort to hospitals of Singapore or US, middle class people in Bangladesh often fail to get adequate treatment in the country. Let alone vulnerable people living in haor or char areas, urban-dwellers often experience tremendous difficulty in accessing government health service marred by corruption.
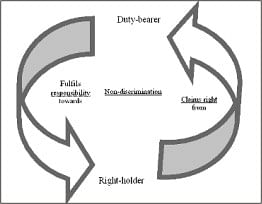 |
Relation between right-holder and duty bearer in a right-based
health service |
Accountability, corruption and the state of health sector
“Making Governance Work for the Poor”, UK government's white paper (http://www.dfid.gov.uk/wp2006/whitepaper-printer-friendly.pdf) on international development reveals that public procurement is a source of corruption. As referred in the document, Transparency International's bribe payers' index suggests that the construction, defence, and health sectors are highly prone to bribery. However, corruption not only occurs in procurement, people often face difficulty in accessing public health services due to widespread corruption and lack of accountability.
World Bank's Country Assistance Strategy (CAS) reveals maternal mortality in Bangladesh is high as a result of inadequate access to health services during pregnancy and childbirth and the poor nutritional status of pregnant women. More than half the children aged 1-3 are underweight and more than 40% women are severely malnourished.
There is a poor accountability mechanism in the health sector as many of us have read in the newspapers about the incident took place in Sylhet M A G Osmani Medical College Hospital a few months back. It has been reported in The Daily Star (April 8, 2008) that 23 patients died since the trouble began after an intern misbehaved with a pregnant woman. These triggered brawls between interns and patients' attendants and later the interns went unruly and swooped on patients' attendants and newsmen at the hospital. Earlier, it has been reported in The Daily Star (April 7, 2008) that some attendants of a pregnant womanRumi Sarker Rumaraised protest as a female intern started checking the lady at an open space and in presence of attendants of other patients at the labour ward. When asked to take the patient inside, intern Alo became angry and knocked the patient on to the floor from the trolley. At about 9 PM Alo, along with some of her fellow interns, went back to the ward and swooped on Ruma's husband Abdullah. It led to further clashes and the internees even launched series of attacks on newsmen too.
The incident mentioned above is part of the scenario that prevails in health sector. Similar incidents also happened in other hospitals, though access to health services is a basic right under international law. Access to health services is a basic necessity set forth in the constitution of our country, nevertheless.
MDG and International Human Rights Instruments
Millennium Development Goals (MDG), which are to be achieved by the target date of 2015, form a blueprint agreed to by all the world's countries and the entire world's leading development institutions. Bangladesh though committed to reach the goals by 2015, has much more to do with health sector. It is particularly important as three (3) goals are directly related to health.
These are Millennium Development Goals related to health care:
* Goal 4: Reduce child mortality
* Goal 5: Improve maternal health
* Goal 6: Combat HIV/AIDS, malaria, and other diseases
 |
Photo: www-cartoonstock-com |
Bangladesh has ratified over 12 UN Human Rights treaties and four optional protocols and also became a member of the UN Human Rights Council in May 2006. It has been stated in Article 25 of Universal Declaration of Human Rights (UDHR), “Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control”.
Again, UN Convention on the Rights of the Child (CRC) lays the responsibility with the state. “States Parties recognize the right of the child to the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health. States Parties shall strive to ensure that no child is deprived of his or her right of access to such health care services” said in Article 24 of CRC.
Moreover, Bangladesh also singed International Covenant on Economic, Social and Cultural Rights (ICESCR).”The States Parties to the present Covenant recognize the right of everyone to the enjoyment of the highest attainable standard of physical and mental health” said in Article 12 of ICESCR.
Furthermore, Bangladesh signed and ratified Convention on Elimination of all forms of Discrimination against Women (CEDAW). Non-discrimination and equal access for both men and women to health services reflected in Article 12(1), “States Parties shall take all appropriate measures to eliminate discrimination against women in the field of health care in order to ensure, on a basis of equality of men and women, access to health care services, including those related to family planning”. State responsibility regarding women health issue is further elaborated in Article 12(2), “Notwithstanding the provisions of paragraph I of this article, States Parties shall ensure to women appropriate services in connection with pregnancy, confinement and the post-natal period, granting free services where necessary, as well as adequate nutrition during pregnancy and lactation”.
Constitution and domestic law
State has responsibility towards citizen in providing health services. It has been stated in Article 15 (a) of the constitution of Bangladesh,” It shall be a fundamental responsibility of the State to attain, through planned economic growth, a constant increase of productive forces and a steady improvement in the material and cultural standard of living of the people, with a view to securing to its citizens the provision of the basic necessities of life, including food, clothing, shelter, education and medical care”.
Though there are no existing laws providing remedies for medical negligence, consumers still can claim compensation. If negligence results in grievous hurt, it is punishable under the Penal Code. It has been asserted in Section 338 of the Code, “Whoever causes grievous hurt to any person by doing any act so rashly or negligently as to endanger human life or the personal safety of others shall be punished with imprisonment of either description for a term which may extend to two years, or with fine which may extend to five thousand taka, or with both”.
When people die due to negligent act, imprisonment might extend to a term of 5 years. “Whoever causes the death of any person by doing any rash or negligent act not amounting to culpable homicide shall be punished with imprisonment of either description for a term which may extend to five years, or with fine, or with both”- said in Section 304(a) of the Penal Code.
Although Bangladesh Medical and Dental Council (http://www.bmdc. org.bd/) was constituted under the Medical and Dental Council Act (Act No. XVI of 1980) to look after public interest, the council has so far failed to convince right-holders of health services. Particularly, there is hardly any evidence where council has acted on public interest if there is a conflict between practitioners and general public.
“Gross negligence in respect of his professional duties to his patient maybe regarded as misconduct sufficient to justify the suspension or the removal of the name of a Medical/Dental practitioner from the Register” stated in Section 5(A) of Code of Medical Ethics.
However, there is little scope for public in existing laws to ensure accountability of health service providers. There are laws and ordinance for specific diseases [like Epidemic Disease Act (1897), Prevention of Malaria Ordinance (1978), Eye Surgery (Restriction) Ordinance (1960)], those laws, nevertheless do not deal with the rights of patients or other stakeholders of health service. Quality of services, therefore, remains poor at Thana Health Complex and even in district hospitals as service providers are not accountable to right-holders.
Scope of work
Bangladesh government is committed to eradicate extreme poverty by 2015 and has prepared poverty reduction strategy. Moreover, international community has committed resources in this regard and UK Department for International Development (DFID) has awarded Harewell International a contract to manage a challenge fund (http://shiree.org) of £65 million aiming at assisting Bangladeshi and international NGOs in the graduation of over 1 million extreme poorest people from poverty by 2015. In supporting the government's reform concept for the public health sector, the EC's overall objective is also to improve the health status of population - particularly the poor, women and children in both urban and rural areas.
NGOs could take this opportunity to organise consumers and right-holders and create a platform to make service providers of health accountable. NGOs nowadays operate clinics in both urban and rural areas and there must be an accountability mechanism in those clinics too. Involvement of civil society organisations, local government representatives, journalists and legal practitioners will strengthen the platform. It might pave the way to accessing health services for extremely poor people.
The writer is human rights worker.







