Dengue virus: once again!
Shakeel Ahmed Ibne Mahmood and Belal Ahmed Ibne Mahmood
Introduction:
The reemergence of the dengue virus has been very dreadful in recent times. The term "Dengue" has its origin in Zanzibar, where the disease was called 'Denga' during the 1870 epidemic as mentioned by N. Haq in an article in 2001.According to WHO , dengue fever is marked by a sudden onset of high fever, severe headache and pain behind the eyes and myalgia / arthralgia. The symptoms and signs may be very similar to other viral infections. It occurs in epidemic form in most countries of Asia and other Pacific islands. Children below 15 years are the common susceptible victims. Dengue epidemic in developing countries is due to many reasons. The disposal of sewage, method of water purification, and most importantly nutritional status of the general population are important reasons for these viral infections. Current situation in Dhaka:
Bangladesh, at the moment, is experiencing this viral infection in a most horrific manner. The number of patients detected with dengue is increasing at an alarming rate, and the Dhaka City Corporation (DCC) is worried that it might turn into an epidemic. According to Daily Star dated July 21, 2006, a survey report of the DCC dengue control section revealed that around 150 government hospitals and private clinics in the capital are presently treating at least 230 dengue patients. The survey also revealed that 31 patients were admitted to different clinics and hospitals in the city on July 19 while 51 patients were admitted the previous day. It was also mentioned that around 408 patients were diagnosed with dengue as of July 22, 2006 in Dhaka. Of them, 178 have been discharged from the hospitals and clinics. There has been no report of deaths so far. This DCC report revealed that two hundred and twenty-three patients had died of dengue during 2000-2005 and 19,551 dengue patients were admitted to clinics and hospitals. Surveying several hospitals and clinics, The Daily Star has found that the number of infant dengue patients is smaller this year than in the previous years Historical Aspects
The classical form of dengue has been known for more than a century in the tropical South East Asia, and Western Pacific Regions. EB Yunus, a dengue expert, mentioned in his article that dengue haemorrhagic fever was reported as a new disease for the first time in the Philippines in 1953. Serotypes 2, 3 and 4 were isolated in 1956. Multiple infections were followed in 1958 in Thailand, in 1970 in Myanmar and finally in India in 1963. In 1965 there was an outbreak of dengue and 'Chikungunga' virus infection called 'Dhaka fever' which was the first documented out-break of dengue in Bangladesh. A WHO sponsored small-scale survey also detected dengue haemorrhagic fever cases in 1982. It is difficult to understand why this virus was reactivated in Bangladesh. Probably seasonal occurrences, such as monsoon-rain, are ideal for breeding. The best environmental conditions for mosquito breeding prevails during pre and post-monsoon periods in the tropical zones. Aedes eggs can survive in dry conditions for a year. WHO estimated that there might be 50 million to 100 million cases of dengue infections worldwide every year. Two fifth of the world's population are at risk of infection. In Bangladesh the last time experienced the worst dengue outbreak, with the majority of cases being in the capital. Thisyakorn U, in his article in 1993, stated that over the last 10-15 years, dengue fever and dengue haemorrhagic fever have become a leading cause of hospitalisation and death among children in South East Asian regions, followed by diarrhoeal diseases and acute respiratory infections. Social and Environmental Aspects
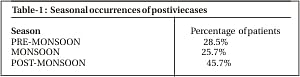
In comparison to malaria, tuberculosis, leprosy, filariasis, diarrhoeal diseases, leishmaniasis, there is no significant differences with dengue infection in Bangladesh. Dengue infection involves mostly the affluent section of the society indicating that it is an urban disease. Usually there is negative correlation between the infection and the undernourished. The peculiarity of the carrier has close link with human habitation. Female Aedes mosquitoes are the carriers of the virus and are peridomestic in nature. The tropical zone of the world, between 350N and 350 S latitude, and area not over 1,000 ft. above sea level is their usual habitat. The areas are marked by monsoon-rains. The breeding of the mosquitoes is highest during pre and post-monsoon periods. Aedes breeds in clean, still and stagnant water usually found in discarded tyres, water tanks and storage appliances which are the ideal sites for breeding. Aedes is a voracious bloodsucker, which helps more virus transmission during blood meal. Biting occurs throughout the day, especially between 8:00 A.M to 13:00 P.M and between 15:00 P.M to 17:00 P.M., therefore late risers and late evening sleepers are more susceptible to mosquito bites. The mosquito sucks blood many times and, therefore, it can infect many persons. Like all carrier-borne diseases, dengue also needs some conducive predisposing conditions for endemicity and outbreaks. According to WHO, the countries of South-East Asia share common features like large populations, rapid urbanisation, development activities and monsoon rains. Urban human populations now constitute the natural reservoir, travelers are the only disseminating factor of the viruses from one country to another. A survey in Dhaka city, by eminent entomologist MA Chowdhury in 2000, discovered that independent houses were most likely to have high densities of Aedes mosquitoes. It appears that the rooftop concrete water containers are one of the main breeding sources in independent houses. EB Yunus showed in his article in, 2000, that in the city of Chittagong from September 1996 to June 1997, among 255 positive cases shows a seasonal variation in Dengue Patients (Table 1). Conclusion:
The prevention of dengue fever is largely based upon the identification of risk factors and awareness. Factors responsible are overpopulation, uncontrolled urbanisation, and inadequate waste management. It is important to bear in mind that the Aedes mosquito is also a carrier for yellow fever. The main threat of yellow fever is the periodic invasion of the virus to densely populated urban areas where it can be transmitted by human biting species. Therefore, it can be anticipated the future impact of this tropical disease in Bangladesh. The most essential step regarding the prevention of this deadly dengue is the indentification of the mode of Aedes mosquito breeding and the method of spraying insecticide/larvaecide at the appropriate sites. Most Aedes mosquitoes breed within houses where the reach of government investigations is limited. The participation and cooperation of the general people with government agencies is essential for Aedes control programs.
|